To receive a free PDF copy of The Fundamentals of Electrocardiograph Interpretation by Harry Mond, subscribe to his email blog by entering your email address below.
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.
Purchase the textbook
Purchase a hard cover or paperback copy of The Fundamentals of Electrocardiograph Interpretation by Harry Mond on Amazon.
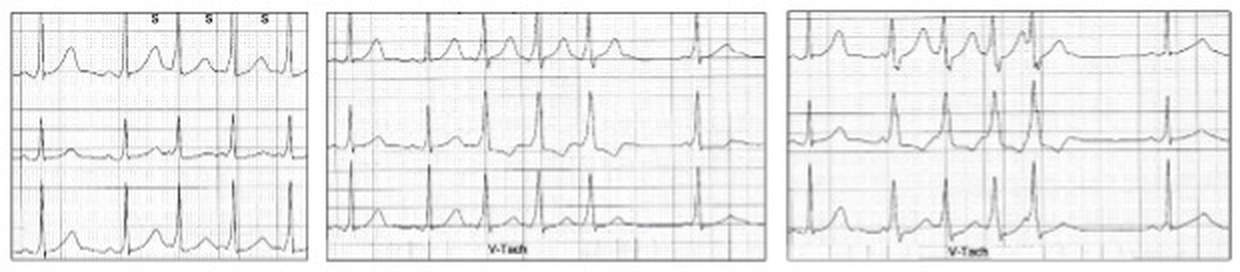
I came upon these ECG tracings of ventricular tachycardia from a Holter study in a 79-year old asymptomatic female.
Analyse each tracing separately.
A clue: I don’t think this is aberrant ventricular conduction
What do you think?
---
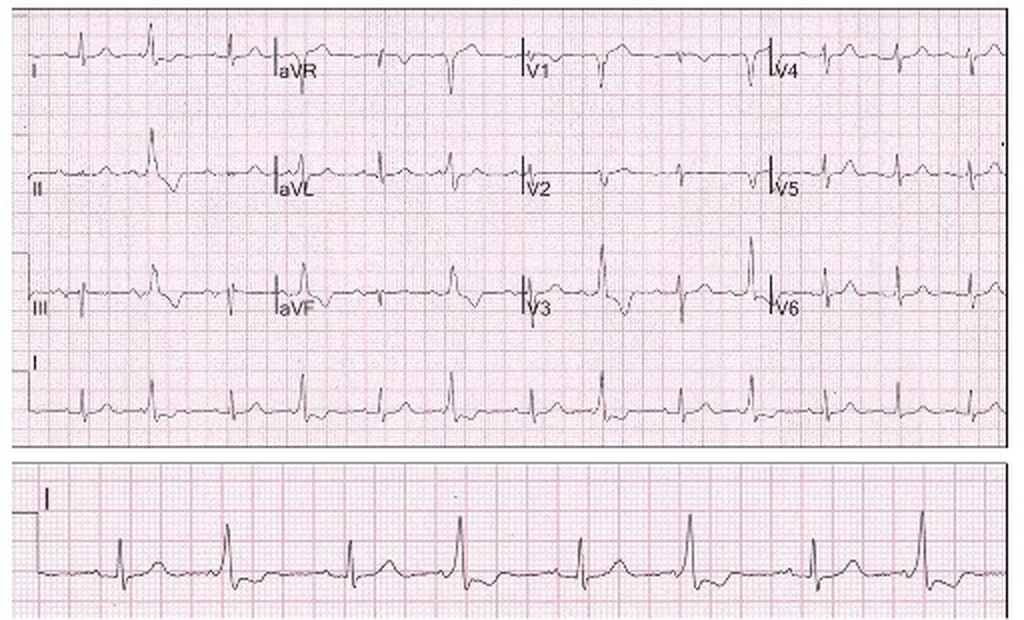
Let us review the baseline ECG:
Sinus rhythm with a short normal PR interval (~120 ms) and a delta ( Δ ) wave (red oval).
Although not easy to see, this suggests pre-excitation in an asymptomatic elderly patient.
Pre-excitation
The ECG features of pre-excitation, commonly known as the Wolff-Parkinson-White (WPW) pattern were first reported by Wilson in 1916, but the relationship to atrial tachyarrhythmias in young adults was by Wolff, Parkinson and White in 1930. The ECG footprints identify a congenital accessory pathway which may lead to reentry tachyarrhythmias, and the syndrome can be associated with a small risk of sudden cardiac arrhythmic death.
When the ECG features are associated with tachyarrhythmias, this is called the “WPW syndrome”. The ECG, however, by itself is said to show “pre-excitation” or a “WPW pattern”. The incidence of pre-excitation is ~ 0.2% of the general population. The pre-excitation reentry circuits also involve the ventricle, but for convenience they are usually described under the heading of supraventricular arrhythmias.
In the normal heart, the fibrous skeleton which supports the heart during contraction also acts as an electrical barrier to conduction from atrium to ventricle, thus directing cardiac conduction to the ventricle via the AV node. The AV node also acts as a gatekeeper delaying conduction via decremental conduction, to allow optimal ventricular filling and this represents most of the PR interval on the ECG.
A congenital, thin filamentous muscular breach of this fibrous skeleton is referred to as the bundle of Kent and is an accessory conduction pathway or bypass tract from atrium to ventricle. It may conduct to the ventricles faster than via the AV node, and thus on the ECG, the PR interval is shortened, and the early ventricular depolarization is seen as a delta (Δ) wave at the commencement of the QRS.
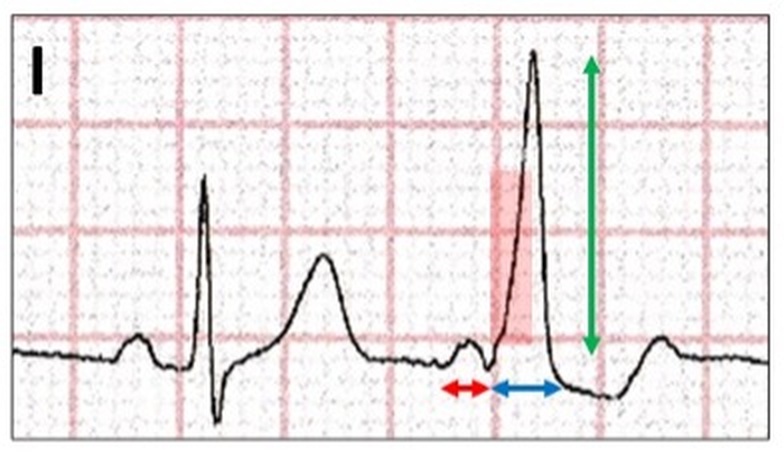
ECG features of an accessory pathway:
Sinus rhythm with normal AV conduction on the left and accessory pathway conduction on the right.
A short PR interval <120 ms, suggesting bypass of the AV node (red arrow).
Δ wave or slurring of the initial QRS denoting the passage of the impulse via the accessory pathway (red highlight).
ST/T wave changes, with the T wave usually discordant with the Δ wave.
(Abnormal depolarization results in abnormal repolarization).
The Δ wave size and morphology vary considerably, depending on the location and conduction of the accessory pathway.
Pre-excitation may alternate with normal AV nodal conduction.
Alternating pre-excitation with a prominent Δ wave. This appearance can be confused with end-diastolic ventricular bigeminy.
Let us return to our case study:
How do we explain the PR interval and modified Δ wave?
With an intact accessory pathway, conduction from a sinus or ectopic atrial site enters both the AV node and accessory pathway almost simultaneously. Because of slow AV nodal decremental conduction, the accessory pathway depolarizes the ventricles first, blocking AV conduction as concealed retrograde conduction.
With altered conduction dynamics such as a relatively “slow” conduction in the accessory pathway, both may contribute to ventricular depolarization resulting in a fused QRS complex. Such pathways may be protected from reentry arrhythmias and although this is often the case, it is important to remember that both anterograde and retrograde conduction are required for reentry and thus anterograde delay in the accessory pathway may not be relevant. It is also important to remember that with atrial fibrillation, accessory pathway conduction may still be rapid and the clinical scenario not necessarily benign.
It may be possible on Holter monitoring to follow the gradual development of the WPW pattern via gradual fusion of both pathway.
Left: Progression from AV nodal conduction with a normal PR interval to a broad QRS and shortened PR interval (very light red highlight).
Middle and right: Gradual widening of the QRS, shortening of the PR interval and development of a more discrete Δ wave (increasing intensity of red highlight).
During short runs of atrial tachycardia, there may be increased conduction via the accessory pathway resulting in a shorter PR interval and increasing prominence of the Δ waves suggesting complex dynamic changes in conduction velocity or refractory periods in either or both conduction pathways.
Sinus rhythm with short runs of atrial tachycardia demonstrating different levels of QRS fusion (S and incorrectly labelled V-tach). There is shortening of the PR interval with an increasing Δ wave excluding aberrant ventricular conduction.
Similarly, changes in PR interval and QRS morphology may follow a compensatory pause with an atrial ectopic
Sinus rhythm with fused QRS complexes. An atrial ectopic results in a compensatory pause and increased accessory pathway conduction with a shorter PR interval and a more prominent Δ wave (red highlight).
or a ventricular couplet.
Summary:
Sinus rhythm with a fused WPW pattern.
The contribution of AV nodal and accessory pathway conduction to the PR interval and QRS morphology may alter with changing conduction dynamics.
No tricks. Just a selection of tracings from a Holter study.Look at each one carefully, use calipers, arrows and highlight and write down your conclusions.