To receive a free PDF copy of The Fundamentals of Electrocardiograph Interpretation by Harry Mond, subscribe to his email blog by entering your email address below.
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.
Purchase the textbook
Purchase a hard cover or paperback copy of The Fundamentals of Electrocardiograph Interpretation by Harry Mond on Amazon.
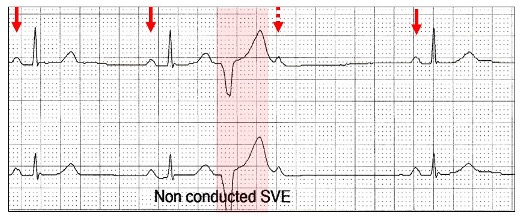
The annotation says “non-conducted supraventricular (atrial) ectopic”.
To summarize: Non-conducted atrial ectopic.
The ectopic P wave is premature (blue arrow).
The ectopic P wave is usually different from the sinus P wave (red arrows).
Sinus cycle is reset after the dropped beat, resulting in a compensatory pause.
The PR intervals before and after the blocked beat are usually the same (red highlight), unless there is concomitant Wenckebach AV block.
Let us return to our tracing.
The major footprints of a non-conducted atrial ectopic have not been fulfilled:
The P wave is not premature and in time with the sinus cycle (red arrows).
The dropped P wave (red stippled arrow) is identical to the sinus P wave.
The sinus cycle has not been reset.
This is not a non-conducted atrial ectopic, but rather sinus bradycardia (red arrows) with a ventricular ectopic (red highlight) and the timing is such that the next sinus P wave is not conducted to the ventricle, because the conducting system is still refractory (red stippled arrow).
With ventricular ectopics (red highlight), the embedded sinus P wave is usually concealed (red stippled arrow)within the ectopic and unlike other sinus P waves (red arrows) does not conduct to the ventricle.
A poorly understood feature of ventricular ectopics is that the non-conducted sinus P wave may not be concealed within the ectopic QRS. With appropriate timing as well as QRS/T length and shape, the sinus P wave may emerge from the tail of the QRS or even the T wave.
Sinus rhythm (red arrows) and two very premature ventricular ectopics (red highlight). At the end of the ectopic QRS, the normally concealed sinus P waves can be seen sticking their noses out (red stippled arrows).
The sinus rate as well as ectopic prematurity play important roles in uncovering the non-conducted P wave.
Here are ECGs from the same patient at different sinus rates.
Sinus rhythm 62 bpm (red arrows) with a ventricular ectopic (red highlight) followed by a non-conducted sinus P wave (stippled red arrow) at the foot of the T wave.
If the rate slows:
The sinus rate is now 50 bpm (red arrows) with a different configuration ventricular ectopic (red highlight) and the non-conducted sinus P wave is later (red stippled arrow), but still within the refractory period of the ectopic. This mimics second degree AV block and hence I call this pseudo AV block. Remember it is physiologic and dependent on the timing of both the sinus rhythm and the ventricular ectopic.
What happens if AV conduction is not refractory?
We then call the ventricular ectopic “interpolated”, as there is no compensatory pause.
Sinus rhythm (red arrows) and a ventricular ectopic (red highlight) with a non-concealed sinus P wave (red stippled arrow) lying outside the refractory period and therefore conducting to the ventricle, albeit with a prolonged PR interval. Although there is no compensatory pause, the R-R interval containing the embedded ectopic is longer (1340 ms) than without (1140 ms) by an amount equal to the lengthening of the PR interval (200 to 400 ms).
No tricks. Just a selection of tracings from a Holter study.Look at each one carefully, use calipers, arrows and highlight and write down your conclusions.
I was asked to review this Holter monitor, the report of which stated: “Sinus rhythm, ventricular rate ~ 90 bpm, Wenckebach AV block”. What do you think?