To receive a free PDF copy of The Fundamentals of Electrocardiograph Interpretation by Harry Mond, subscribe to his email blog by entering your email address below.
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.
Purchase the textbook
Purchase a hard cover or paperback copy of The Fundamentals of Electrocardiograph Interpretation by Harry Mond on Amazon.
Two rhythm strips from a Holter monitor recording: Same patient, seven hours apart.
Both, (red and yellow highlight) have been given the annotation “SVE Pair”; supraventricular ectopics in a pair or in other words, atrial couplets. What do you think? Look at the tracings carefully and remember “It’s all in the timing”. In order to explain what is going on, we need to return to the basic timings of atrial ectopy. The term “ectopy” refers to ectopics including all groupings such as couplets.
An atrial ectopic (red highlight) has three features: • A premature P wave. This may be absent (junctional) or buried in the previous T wave (concealed). It may be similar to the sinus P wave (site crista-terminalis) or different (ectopic atrial focus). • The subsequent QRS is usually conducted with a normal or near-normal appearance. If wide, then there is aberrant conduction. If AV conduction is totally refractory, then it is a non-conducted atrial ectopic. • Following the T wave, there is a compensatory pause, which is measured to the P wave of the next beat. If absent, then the ectopic is interpolated.
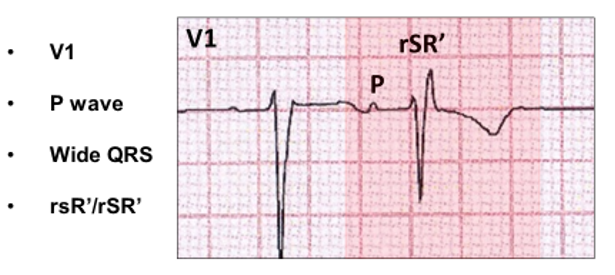
A few words on ventricular aberration: Aberrant conduction results from intermittent uneven physiologic refractoriness in the ventricular conducting system from an early supraventricular focus. There is QRS widening, consequent to a delay or block in one of the bundle branches (usually right) or a more peripheral branch.
Ventricular aberration can be explained as follows:
This is the classical ECG appearance of aberrancy (red highlight):
The compensatory pause can be either full or partial.
I have never found an explanation in the literature, so this is my explanation.
Full compensatory pause:
The atrial ectopic (red highlight) appears to interrupt the regular sinus cycle (red vertical arrows). Following the atrial ectopic, the next sinus P wave is concealed in the ectopic T wave (blue arrow) and thus the timing of the sinus cycles are not interrupted. For a full compensatory pause, two sinus cycles (red horizontal arrows) with the embedded atrial ectopic (1640 ms) are near identical to two sinus cycles without an atrial ectopic (1660 ms).
Partial compensatory pause:
The sinus cycle timing (red vertical arrow 350 ms) is interrupted by the atrial ectopic (red highlight). The next sinus P wave (blue stippled vertical arrow) is refractory due to retrograde conduction (green vertical arrow). The timing of the next sinus beat (stippled red vertical arrow) occurs 1350 ms after the green arrow. For a partial compensatory pause, the two sinus cycles with the embedded atrial ectopic is shorter (2000 ms) than without the ectopic (2700 ms). An interpolated atrial ectopic (red highlight) occurs when the next sinus cycle (blue vertical arrow) is not refractory allowing conduction to the ventricle (yellow highlight) thus obliterating the compensatory pause.
Note that the atrial ectopic demonstrates minor aberration.
Timing is critical for interpolation.
Tracings are from the same patient taken minutes apart. Note first degree AV block.
In figure A, the atrial ectopic (red highlight) occurs 660 ms after the previous sinus beat (red vertical arrow). The next sinus P wave is concealed in the ST segment (blue vertical arrow) and does not conduct resulting in a compensatory pause. In figure B, there is interpolation. The atrial ectopic (blue highlight) occurs earlier (460 ms) and now the next sinus P wave (green arrow) is concealed within the ectopic T wave, allowing AV conduction with a longer PR interval.
Not all interpolation is true interpolation!
This ECG mimics an atrial ectopic (red highlight) with interpolation and aberration (V1 is a right bundle branch block configuration).
There are however, important differences; the sinus cycle is 1220 ms, yet the cycle with the embedded atrial ectopic is shorter (1080 ms) and the subsequent P wave is inverted. This is an echo beat (yellow highlight) and because it is marginally later than the atrial ectopic conducts without aberration.
Two consecutive atrial ectopics (red highlight) without an intervening sinus beat is a couplet (blue vertical arrows).
Not all atrial couplets (red highlight) are premature (blue vertical arrows).
Not all atrial couplets (red highlight) conduct to the ventricle (blue vertical arrows).
There is a Wenckebach AV block sequence within the couplet. Not all atrial couplets are couplets:
In this tracing, the P wave (blue highlight) before the two atrial ectopics (red highlight) has a different P wave morphology to the other sinus beats and is marginally premature (red horizontal arrows). This is atrial fusion, an amalgam between a very late atrial ectopic and a sinus P wave, a few milliseconds later. This is an atrial triplet or three consecutive atrial ectopics.
Now we know everything about atrial ectopy, let us return to our original “SVE pairs”.
Atrial triplet! The first complex (blue highlight) is an atrial fusion beat.
Interpolated atrial ectopic. The timings and appearance of the P waves confirm this.
I was asked to review this Holter monitor, the report of which stated: “Sinus rhythm, ventricular rate ~ 90 bpm, Wenckebach AV block”. What do you think?