To receive a free PDF copy of The Fundamentals of Electrocardiograph Interpretation by Harry Mond, subscribe to his email blog by entering your email address below.
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.
Purchase the textbook
Purchase a hard cover or paperback copy of The Fundamentals of Electrocardiograph Interpretation by Harry Mond on Amazon.
Let us commence by reviewing a few basic principles of ECG interpretation.
Principle 1. Junctional (or atrial) ectopics.
We have previously described three types of junctional ectopics:
P wave embedded in the QRS
P wave following the ectopic QRS
Inverted P wave preceding the ectopic QRS.
Inverted P wave precedes the QRS: The pacemaker focus is high in the AV junction allowing the retrograde wave to depolarize the atria first (red highlight, red half circle), then traverses theAV junction anterograde, before depolarizing the ventricle.
If the ectopic is late, the next sinus P wave may not conduct to the ventricle.
Sinus rhythm (red lines), first degree AV block and a late junctional ectopic (blue line, red highlight) immediately before the next sinus P wave, which is inhibited (red stippled line). The following sinus P wave lies beyond the ectopic T wave and AV conduction is still refractory, so it is not conducted resulting in a long “pseudo”compensatory pause. This is frequently misinterpreted as non-conducted atrial ectopics or Wenckebach AV block.
Principle 2. Atrial ectopics may conduct to the ventricle with aberrancy.
The premature junctional ectopic is conducted with a broad QRS or aberrant ventricular conduction (red highlight).
Principle 3. Supraventricular rhythms may conduct to the ventricle with a bundle branch block, which may berate dependent.
Sinus rhythm with a bundle branch block when the sinus cycle is 800 ms (75 bpm). When the sinus rate slows to 66 bpm (900 ms), AV conduction becomes normal. This is referred to as a rate dependent bundle branch block.
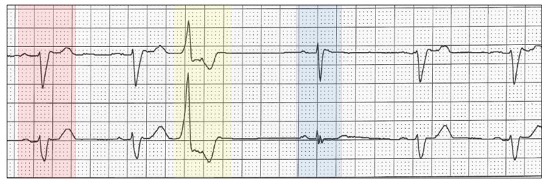
Principle 4. ECGs with a bundle branch block may demonstrate QRS narrowing, immediately after the compensatory pause.
The same principle can be applied to the compensatory pause. Sinus rhythm conducted with a bundle branch block (red highlight). A ventricular ectopic (yellow highlight) is followed by a partial compensatory pause and the next sinus cycle is conducted with a narrow QRS (blue highlight), suggesting that the bundle branch block is rate dependent.
Here is another example.
Sinus rhythm with bundle branch block (red highlight). An atrial couplet (yellow highlight) results in a compensatory pause and the next sinus beat conducts with a narrow QRS.
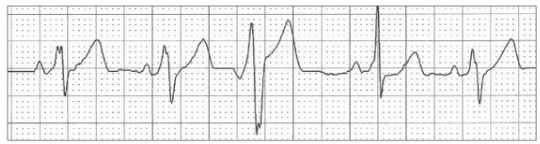
Now let us return to our ECGand using the principles espoused, diagnose the tracing.
Sinus rhythm (red lines), rate 76 bpm (760 ms)conducted with a bundle branch block (red highlight).
Late junctional ectopic (blue line) with aberrant ventricular conduction (yellow highlight) with the next sinus P wave inhibited (red stippled line).
Following a minor compensatory pause (840 ms),the sinus beat now conducts with a normal width QRS (blue highlight).
The critical timing has resulted in two types of broad QRS complexes:
No tricks. Just a selection of tracings from a Holter study.Look at each one carefully, use calipers, arrows and highlight and write down your conclusions.
I was asked to review this Holter monitor, the report of which stated: “Sinus rhythm, ventricular rate ~ 90 bpm, Wenckebach AV block”. What do you think?