To receive a free PDF copy of The Fundamentals of Electrocardiograph Interpretation by Harry Mond, subscribe to his email blog by entering your email address below.
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.
Purchase the textbook
Purchase a hard cover or paperback copy of The Fundamentals of Electrocardiograph Interpretation by Harry Mond on Amazon.
This ECG was sent to me by Ken at Cardioscan Melbourne.
Thank you Ken.
What do you think?
This is one of those “nonsense” looking pacing ECGs that doesn’t make sense but is identified by “instant recognition”.
The clues:
Atrial pacing (or sensing).
Very long PR interval.
A non-conducted atrial paced (or sensed) beat
Followed by atrial pacing/ventricular pacing with a very short AV delay.
Let us examine the tracing in detail.
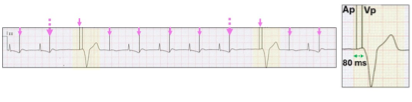
Atrial pacing (70 bpm).
The appearance is confusing because most atrial stimulus artefacts (pink arrows, Ap) lie in the T wave of the previous QRS.
Very long PR interval and sinusoidal P waves.
Following each atrial stimulus artefact, there is a P wave confirming atrial capture (red stippled oval) followed by AV conduction with an excessively long PR interval of 560 ms (green stippled arrows). Not all P waves conduct to the ventricle (red highlight).
Atrial and ventricular pacing with a very short AV delay.
Following failed AV conduction, there is atrial and ventricular pacing (Ap Vp) with an 80 ms AV delay.
This appearance is due to a ventricular pacing minimization algorithm called Managed Ventricular Pacing (MVPTM) - Medtronic Inc. Minneapolis MN, USAand is the easiest and most characteristic of these algorithms to recognise on the ECG.
Why minimize ventricular pacing?
It is now recognised that right ventricular pacing may over time result in left ventricular dysfunction. Consequently, there has been a concerted effort to minimize right ventricular pacing in patients who may not require it. This has resulted in a range of proprietary algorithms, that effectively pace AAI(R), but in the event of failed AV conduction will convert to dual chamber-ventricular pacing. After a set or programmable period, successful scheduled conduction testing will once again allow the pacemaker to pace AAI(R). All these algorithms create bizarre ECG appearances that appear to violate the traditional rules regarding the AV delay and the lower rate limit. Consequently, pacemaker malfunction may be suspected.
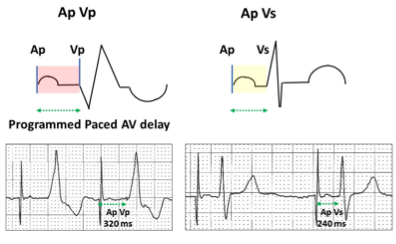
The law of AV conduction as it applies to dual chamber pacing.
The programmed paced AV delay (Ap Vp, red highlight) is always longer than when an intervening conducted QRS terminates it (Ap Vs, yellow highlight).
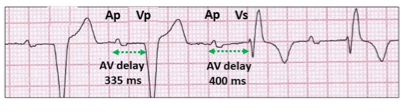
Violation of the law of AV conduction as it relates to ventricular minimization algorithms.
The programmed AV delay is a long 335 ms. AV conduction is allowed to continue to 400 ms as part of the conduction test of the algorithm.
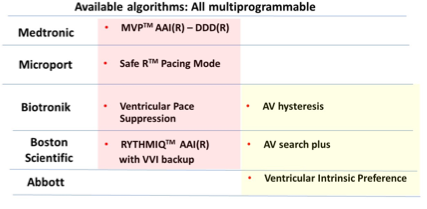
Ventricular pacing minimization algorithms intentionally violate the law of AV conduction in order to encourage ventricular sensing and can be recognised on the ECG by the AV delay being longer than the programmed AV delay. There are currently seven unique algorithms from five manufacturers.
These programmable algorithms can be divided into two broad groups, four convert from atrial to dual chamber pacing (red highlight) in the presence of failed AV conduction allowing pauses and three use AV hysteresis in the DDD(R) mode (yellow highlight). As the name implies, AV hysteresis allows the AV delay to be extended by a given value in order to encourage ventricular sensing. The algorithms can be complex and there are frequent manufacturer software iterations. Generically, on the ECG, there is AAI(R) pacing in patients with intact AV conduction. AV conduction is continually being monitored. In the event of failure of AV conduction, ventricular pacing is triggered and a change in pacing from AAI(R) to DDD(R) pacing is referred to as “mode conversion”.
MVP: Failure of AV conduction during AAI(R) pacing requires a specific number of events for algorithm-offset and conversion to DDD(R) pacing. If failure of AV conduction occurs for one cycle, then the next atrial paced event is followed by ventricular pacing with a short 80 ms AV delay. There are many scenarios that may trigger the algorithm but not initiate ventricular pacing which requires a sequence of events.
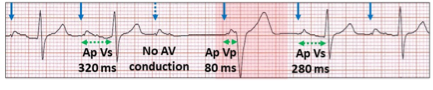
Nocturnal Wenckebach AV block.
Atrial pacing (blue arrows, Ap), ventricular sensing (Vs) and a non-conducted atrial paced beat. (blue stippled arrow). The next Ap Vp has an 80 ms delay (red highlight). There is mode conversion for one cycle, but no algorithm-offset.
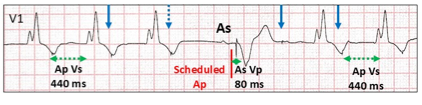
Sinus escape. The 80 ms AV delay is timed to atrial (A-A) pacing, so with atrial sensing, the P wave may be earlier and thus the 80 ms AV delay cannot commence until the next scheduled Ap, the longer AV delay encouraging AV conduction.
Atrial pacing (blue arrows, Ap), ventricular sensing (Vs) and a non-conducted atrial paced beat (blue stippled arrow). A sinus escape beat occurs before the next scheduled atrial paced (Ap) beat. The timing of the 80 ms AV delay does not commence until the next scheduled Ap resulting in a longer AV delay but still considerably shorter than the AV delay with Vs.
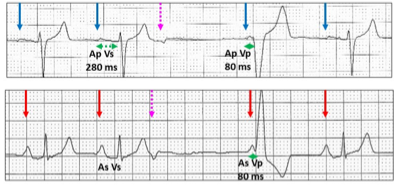
Non-conducted atrial ectopic. The atrial ectopic does not conduct and the algorithm responds with an 80 ms AV delay.
Atrial pacing (blue arrows, Ap) and sinus rhythm (red arrows, As) with ventricular sensing (Vs) and sensed non-conducted atrial ectopics (pink stippled arrows). The next P wave is either As or Ap, but both have an 80 ms AV delay because the scheduled Ap cycle has been completed.
Premature ventricular ectopic.
Atrial pacing (blue arrows, Ap) with ventricular sensing (Vs) and a premature ventricular ectopic (yellow highlight). There is no interruption of the atrial pacing cycle, but ventricular conduction is refractory thus triggering an AV delay of 80 ms.
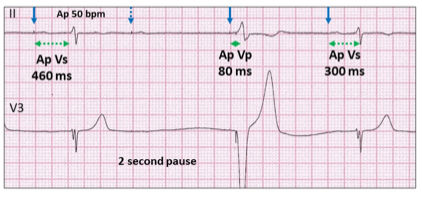
Inappropriate programming. With continual Wenckebach AV block and low atrial pacing rates, minimal ventricular pacing algorithms may result in frequent symptomatic pauses.
Atrial pacing 50 bpm (blue arrows, Ap), ventricular sensing (Vs) with a Wenckebach AV sequence and a non-conducted atrial paced beat. (blue stippled arrow). The next Ap Vp has an 80 ms delay (red highlight). The slow atrial pacing rate and the non-conducted P wave result in a significant ventricular pause.
A single failure of AV conduction will not trigger DDD(R) pacing. This will only occur if two of four consecutive cycles have failure of AV conduction.
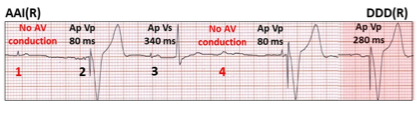
Atrial pacing, ventricular sensing (Ap Vs). Two episodes of AP with failed AV conduction (1 and 4 in red), both followed by Ap and ventricular pacing (Vp) with an 80 ms AV delay.Two of four consecutive cycles have failure of AV conduction and thus there is conversion to DDD(R) pacing (red highlight) at the programmed AV delay.
Although ventricular pacing minimization algorithms are very successful in minimizing ventricular pacing and thus hopefully preserving left ventricular function, this however has been at the expense of creating inappropriate unphysiologic PR intervals and AV delays.
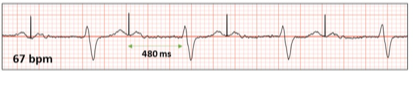
DDDR pacing with a non-AV hysteresis ventricular rate minimization algorithm turned ON allowing the AV delay to extend to 480 ms following atrial pacing. At rest (rate 67 bpm), the atrial stimulus artefact falls at the end of the T wave and with exertion may fall within or even before the T wave. This will result in the atrium contracting at the end of ventricular systole with closed AV valves. Not only is there loss of the atrial contribution to ventricular filling but also retrograde pulsatile pulmonary venous flow which may result in dyspnoea.
In summary, therefore our ECG demonstrated the Medtronic MVP algorithm.
The operation of the algorithm was appropriate with no pacemaker malfunction and both atrial pacing and ventricular pacing identified.
There was atrial pacing at a satisfactory rate (70 bpm) but with a very long inappropriate non-physiologic PR interval (560 ms).
Atrial contraction would have occurred during ventricular systole, thus creating a “pacemaker syndrome”.
There was intermittent failure of AV conduction with triggering of atrial and ventricular pacing with a very short 80 ms AV delay.
There were no two failed AV conductions over four atrial paced beats, which would have allowed conversion to a more physiologic programmed atrial/ventricular pacing.
No tricks. Just a selection of tracings from a Holter study.Look at each one carefully, use calipers, arrows and highlight and write down your conclusions.