To receive a free PDF copy of The Fundamentals of Electrocardiograph Interpretation by Harry Mond, subscribe to his email blog by entering your email address below.
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.
Purchase the textbook
Purchase a hard cover or paperback copy of The Fundamentals of Electrocardiograph Interpretation by Harry Mond on Amazon.
I came across these two tracings from the same patient during Holter reporting.
Do you agree with the reported diagnoses?
---
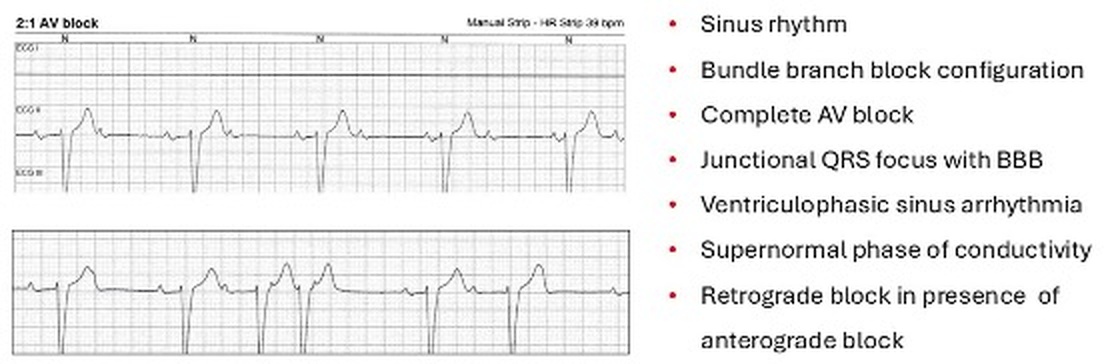
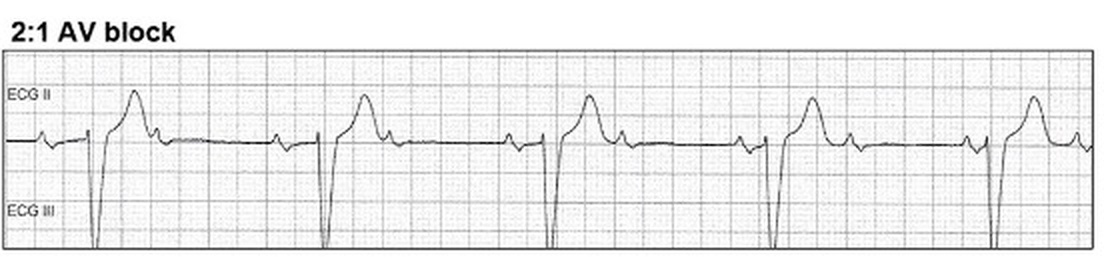
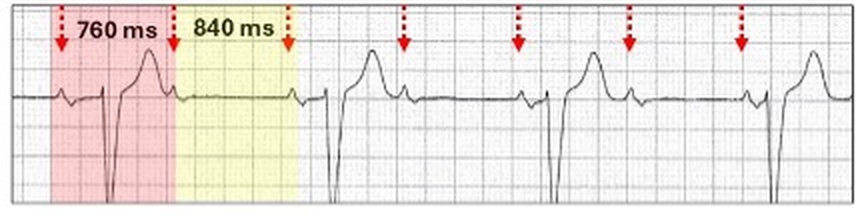
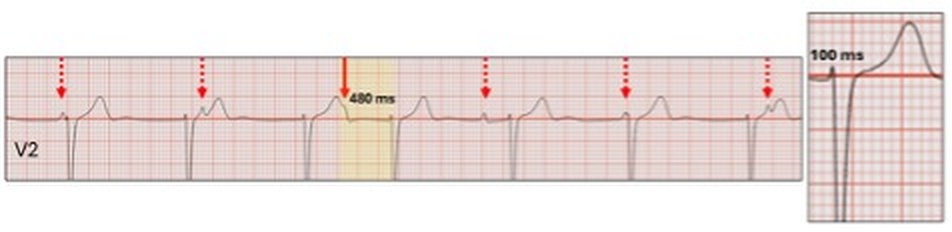
Let us start by reviewing the first tracing.
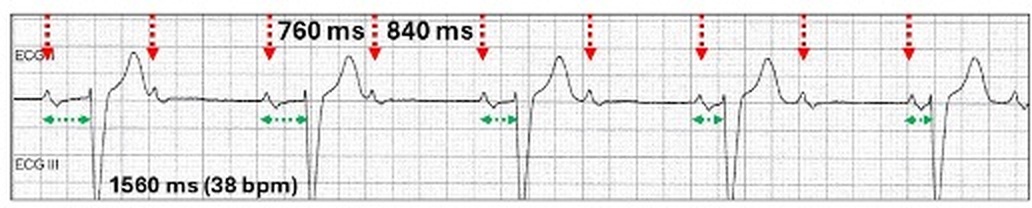
Every second P wave is clearly non-conducted (red stippled arrows) and the ventricular rate is 38 bpm but is this 2:1 AV block?
The PR intervals progressively shorten.
Could this be a reverse Wenckebach AV block?
Tell me about reverse Wenckebach AV block?
Reverse Wenckebach AV block
Rather than PR prolongation, there are repeated sequences of PR shortening and no dropped beats. This may be coupled with non-conducted P waves such as 2:1 AV block and syncope, suggesting advanced conduction tissue disease. On other occasions, the features appear benign on Holter monitoring.
The sequence (red highlight) commences with a very long PR interval which shortens (green stippled arrows) over the next two sinus cycles and then recommences without a dropped beat. The pauses are related to marked PR prolongation with the first beat of the sequence.
For those that think this is complete AV block, the sequences are repeated and the QRS complexes are very irregular.
Our tracing could not be reverse Wenckebach AV block as the PR shortening occurs with each alternate beat.
The diagnosis is sinus rhythm (red stippled arrows) with broad complex complete AV block and the PR relationship is purely fortuitous in this strip with the QRS cycle length (1560 ms, 38 bpm) marginally faster than two sinus cycles.
There is another finding in this tracing.
The P-P cycle length with an embedded QRS (760 ms) is shorter than the P-P cycle length without a QRS (840 ms).
This is ventriculo-phasic sinus arrhythmia.
Ventriculo-phasic sinus arrhythmia
This physiological feature is often overlooked when interpreting ECGs. It is simply variations in the sinus rate, depending on whether there are QRS complexes embedded between sinus cycles. The R-R intervals are shorter with the embedded QRS as there is a cardiac output and the next P-P cycle lengthens (sinus rate slows) as a result. The changes in the sinus rate are seen in ~ 50% of cases of second degree or complete AV block and are reflex mediated through intracardiac and in particular, atrial pressures and volumes.
Wenckebach AV block
2:1 AV block
Complete AV block
Interpolated ventricular ectopics
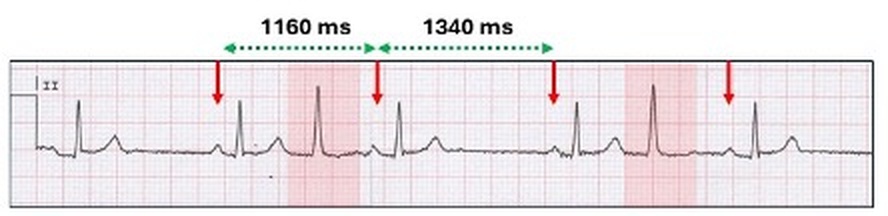
Although ventriculophasic sinus arrhythmia is usually described with AV blocks, interpolated ventricular ectopics create the same physiological milieu and are thus associated with P-P variation.
Sinus rhythm (red arrows) with interpolated fascicular) ventricular trigeminy (red highlight). The P-P intervals with the embedded fascicular ectopics (1160 ms) are shorter than the P-P intervals without the ectopics (1340 ms).
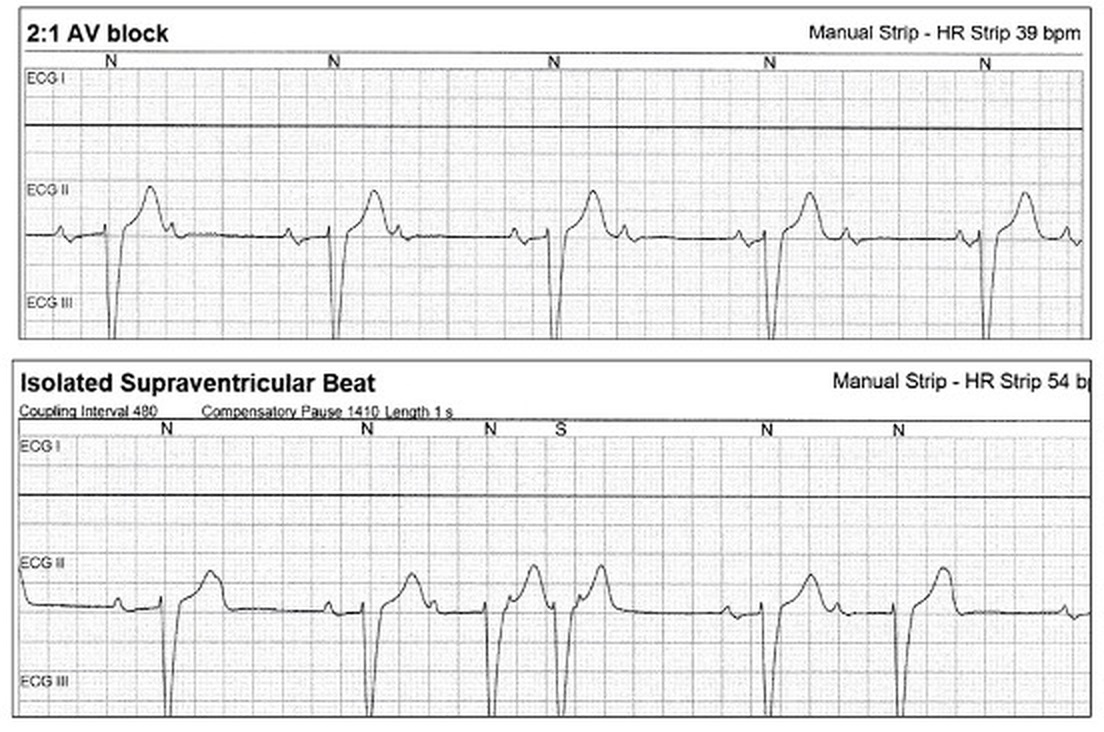
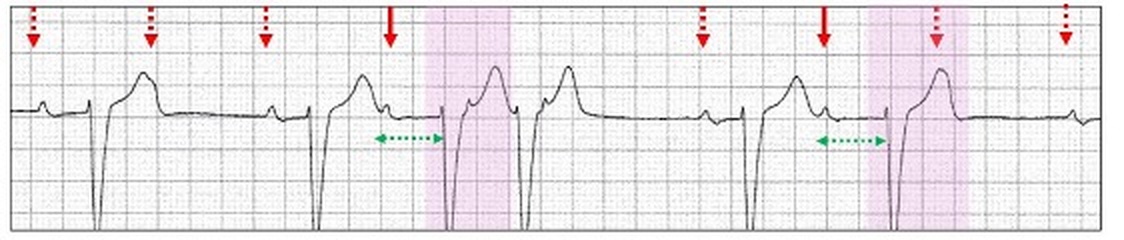
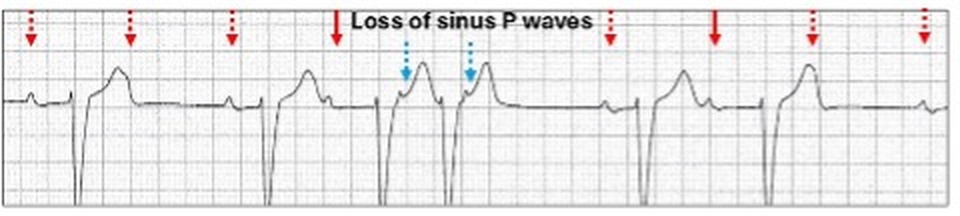
Let us now review the second tracing.
Remember the diagnosis is complete AV block.
The feature of this tracing is the irregularity of the QRS complexes despite complete AV block. How do we explain this?
There are two “premature complexes (purple highlight) with the P waves preceding them lying at the foot of the downslope of the previous T wave.
Despite being complete AV block, these two premature QRS complexes are conducted (red solid arrows).
This is due to supernormal phase of conductivity.
Supernormal phase of conductivity
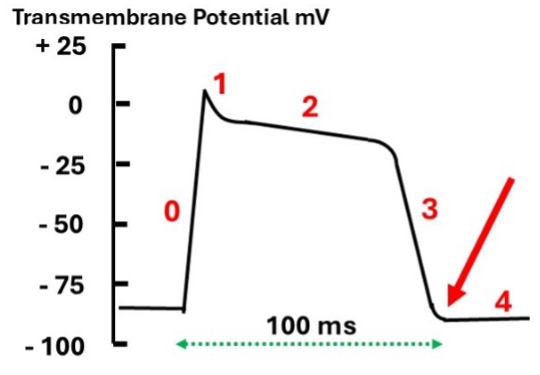
When reviewing long rhythm strips of complete AV block, isolated single episodes of AV conduction can on occasion be seen. This is due to enhanced AV conduction during the supernormal phase (period) of conductivity. The supernormal phase is a very narrow zone within the cardiac action potential just beyond the vulnerable period of the relative refractory period where phase 3 merges into phase 4 (red arrow).
With complete AV block, a propagating wave of depolarization upon reaching the area of block may now be conducted to the ventricle. Supernormal phase of conductivity can be recognized by three features:
The conducted P wave lies at the foot of the previous T wave.
The conducted PR interval is usually (but not always) prolonged.
The conducted QRS is premature compared to the otherwise stable slow ectopic ventricular rhythm.
The pattern of AV conduction is dependent on the underlying pathology with the conducted QRS narrow or broad. By comparing the morphology of the conducted and ectopic QRS complexes, the site of the ectopic focus can be determined.
Narrow conducted QRS (≤ 120 ms)
Sinus rhythm (red arrows) with complete AV block (stippled red arrows) and a slow narrow QRS escape rhythm, suggesting that the pacemaker escape focus is in the AV junction. An identical premature QRS complex (solid red arrows) occurs when the P waves falls in the supernormal phase and conducts to the ventricle along the same conduction pathway.
Broad conducted QRS (≥ 120 ms)
Broad escape ventricular QRS complexes may originate anywhere below the His bundle. The QRS complexes of the escape rhythm and conducted beats bear no resemblance to each other. In this situation, supernormal phase of conduction may be incorrectly diagnosed as ventricular ectopics. Look for the P wave (red solid arrow).
Complete AV block with a broad QRS from an ectopic site in the left ventricle (right bundle branch block configuration) and the conducted QRS has a left bundle branch block with the focus in the right ventricle (red highlight).
In most cases the conducted QRS complex is premature. If, however, the conducted PR interval is very long, then the QRS cycle length may appear regular.
Complete AV block with a broad QRS escape focus from within the ventricle but the conducted QRS has a narrow QRS and because of the long conducted PR interval, the pause appears obliterated.
There is a third scenario where both the ectopic focus and conducted beats have the same broad QRS configuration.
Sinus rhythm with broad complex QRS complete AV block (red stippled arrows). The two conducted QRS complexes (red highlight, red solid arrows) are identical to the ectopic focus. In this situation the focus is in the AV junction, and both complexes are conducted to the ventricles with a bundle branch block.
The concept of supernormal phase of conductivity creates a conundrum. In its definition, complete AV block, unlike high degree AV block, has no AV conduction. When discussing supernormal phase of conductivity, it is best to allow the term complete AV block to be retained. Hence, some reporters prefer the term third degree AV block which would incorporate supernormal phase of conductivity.
Let us return to our second ECG.
There is a break in the sinus rhythm with a loss of P waves. This is because there is “premature” retrograde conduction (blue stippled arrows) from two of the QRS complexes; one sinus generated and one ectopic focus.
If there is complete AV block anterograde, then one would expect it to also demonstrate retrograde (VA conduction) block. In studies with complete AV block, retrograde VA conduction, however, occurs in about 10% of cases and some authorities believe that the anterograde and retrograde pathways are different. Think dual AV nodal pathway physiology!
Here is such an example:
Single chamber ventricular pacing (VVI) in a patient with complete AV block.
With each paced QRS complex, there is retrograde (VA) conduction resulting in a reversed P wave (purple stippled arrow).
The question remains that this retrograde conduction in our case study occurs during the supernormal phase of conductivity and does this play a role in the retrograde conduction?
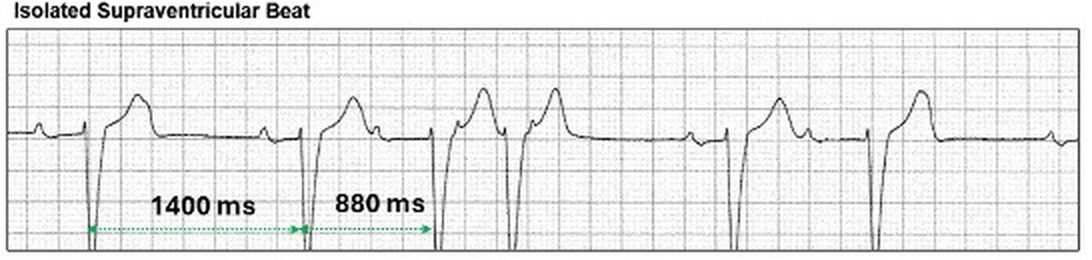
Finally, we have to explain what was called the “Isolated Supraventricular Beat” (red oval).
Mapping out the QRS complexes from the ectopic focus in the AV junction (purple arrows) demonstrates that this very premature beat is from the ectopic focus. There is no QRS complex following the second conducted beat as it falls in the refractory period (blue stippled ghosted arrow).
I was asked to review this Holter monitor, the report of which stated: “Sinus rhythm, ventricular rate ~ 90 bpm, Wenckebach AV block”. What do you think?









.png)