To receive a free PDF copy of The Fundamentals of Electrocardiograph Interpretation by Harry Mond, subscribe to his email blog by entering your email address below.
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.
Purchase the textbook
Purchase a hard cover or paperback copy of The Fundamentals of Electrocardiograph Interpretation by Harry Mond on Amazon.
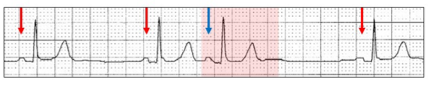
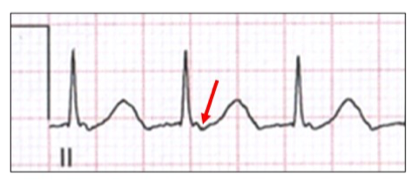
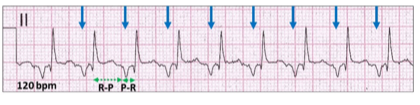
Sinus bradycardia, 50 bpm (red arrows). You got that right!!!
Premature atrial ectopic (blue arrow).
Conducts to the ventricle with a long PR interval of 360 ms (red highlight).
Dual AV nodal pathways physiology is exposed, with slow pathway AV conduction (S). See Fun with ECGs 153.
Let us review how an atrial ectopic can conduct via the slow pathway.
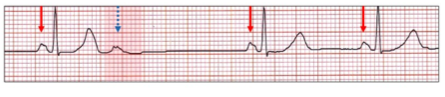
A premature atrial ectopic (blue arrow, red highlight) conducts to the ventricle via the fast pathway with a normal PR interval similar to the sinus beats (red arrows).
If the atrial ectopic is too premature, the fast pathway may be refractory and the ectopic, non-conducted (blue stippled arrow, red highlight).
However, if dual AV nodal pathway physiology is active, an atrial ectopic with a short P-P coupling interval conducting to the ventricle and blocked by the fast pathway may now be able to conduct via the slow pathway.
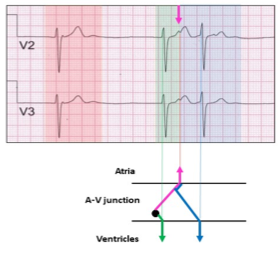
Left: Atrial ectopic (red highlight, blue arrow) with short PR interval and atrial coupling interval of 800 ms.
Right: With shortening of the atrial coupling period (700 ms), the atrial ectopic red highlight, blue arrow) would normally be non-conducted due to a refractory fast pathway. However, the ectopic now conducts through the slow pathway. Also consider concealed retrograde penetration of the proximal conducting system.
Let us return to our case study.
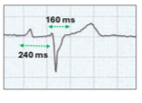
The atrial ectopic does not have a compensatory pause as there is retrograde conduction to the atrium via the fast pathway (F) which is now non-refractory. The result is an inverted P wave (light blue arrow) which in turn conducts to the ventricle via the slow pathway (yellow highlight). This is referred to as an echo beat.
Echo or reciprocal beats are propagating electrical complexes that return and reactivate their site of origin. For teaching, it is easier to remember or say echo beats, although reciprocal beats are a more precise description. They are great mimickers and can be very hard the diagnose even when the footprints are recognised. For this reason, echo beats are frequently missed or more likely misdiagnosed. The most common initiating focus is a junctional ectopic or junctional rhythm although atrial ectopics or ectopic atrial rhythms, ventricular ectopics including ventricular pacing and sinus rhythm with a prolonged PR interval may all initiate echo beats. To generate an echo beat, the impulse must be propagated retrograde and then anterograde. In order to do this, dual AV nodal pathways with differing refractory periods and conduction speeds may be required. A single reentrant conducted atrial complex is seen as an echo beat, whereas a continual circus movement is a reentrant rhythm or tachycardia.
Let us review the mechanism using a junctional ectopic.
Slow junctional rhythm without retrograde conduction (red highlight).
The next complex (green highlight) has both anterograde conduction to the ventricle and retrograde conduction to the atrium (pink arrows).
The atrial impulse can now conduct anterograde to the ventricle via the previously blocked and now non-refractory AV pathway (blue arrow, blue highlight), resulting in an echo beat (blue highlight).
Atrial ectopic.
In order for an atrial ectopic to generate an echo beat, the ectopic should be very premature and the atria non-refractory to the retrograde conduction. The mechanism is again retrograde conduction and dual AV nodal pathways. It may be impossible to differentiate echo beats from either atrial couplets or atrial interpolated beats and the diagnosis depends on differing P waves, which is usually very subtle.
Sinus rhythm and an atrial ectopic (yellow highlight) with an upright P wave (blue arrow, yellow highlight). Earlier in the tracing, an atrial ectopic (red highlight) is followed by a beat with an inverted P wave (pink arrow) and likely to be an echo beat.
Let us return to our case study and follow this through.
The echo beat has created a re-entry circuit (yellow highlight).
The atrial ectopic conducts along the slow pathway (S1).
Because it is now non-refractory, there is retrograde conduction along the fast pathway (F1), which depolarizes the atrium (light blue arrow).
This in turn, conducts anterograde along the slow pathway (S2) depolarizes the ventricle and once again is conducted retrograde (F2), creating a re-entry circuit (S3, F3, S4).
Following AV conduction (F4), retrograde conduction along the fast pathway to the atrium fails because this pathway is now refractory probably because of an increase in the P-P interval from 90 to 100 bpm.
This is an example of a re-entrant rhythm being generated with dual AV nodal pathways. By definition it is not a re-entrant tachycardia as the rate is too slow. How do we explain the slow re-entrant rate? On review of the sinus beat there is both first degree AV block and a bundle branch block suggesting conduction system disease and reduced conduction velocities.
As we are discussing re-entrant rhythms, we should also briefly discuss atrioventricular nodal re-entrant tachycardia (AVNRT) which is the bread and butter of investigative electrophysiology but bewildering to most other cardiologists.
AVNRT is the most common of the regular narrow complex tachycardias and is dependent on dual AV nodal pathway physiology which describes the influence these pathways have on the genesis, analysis, and management of patients with junctional dysrhythmias. The electrical properties are also modified by the autonomic nervous system and pharmacological agents. Atrial and ventricular ectopics, by creating echo beats can provide the milieu for AVNRT.
Atrial ectopy:
As we have previously shown, when one or more premature atrial ectopics reaches the AV node, the fast pathway may be refractory and therefore conduction occurs via the slow pathway. The result is an ectopic beat (blue arrow) with a long PR interval (green stippled arrow).
However, the fast pathway may now be able to conduct retrograde to the atrium, which if electrically recovered, may create an echo beat.
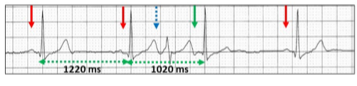
Sinus rhythm (red arrows) with an aberrantly conducted atrial ectopic with the P wave concealed in the previous T wave (blue stippled arrow). There is retrograde conduction with the P wave (green arrow) conducting to the ventricle as an echo beat. The R-R timing (1020 ms) is shorter than the sinus cycle confirming that this is not an interpolated atrial ectopic.
Ventricular ectopy:
If a ventricular ectopic enters the AV node, it may be conducted retrograde to the atrium by the slow pathway if the fast pathway is still refractory.
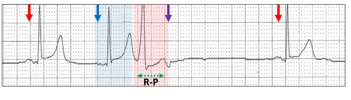
Sinus rhythm (red arrow), followed by a junctional or ectopic atrial beat (blue highlight, blue arrow). A ventricular ectopic (red highlight) conducts retrograde via the slow pathway resulting in an inverted blocked P wave (purple arrow), There is a long R-P interval (green stippled arrow).
If the fast pathway has now recovered, then there is anterograde conduction to the ventricle, creating an echo beat.
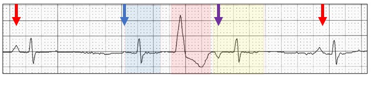
Sinus bradycardia (red arrow), followed by an escape junctional or ectopic atrial beat (blue highlight, blue arrow). A ventricular ectopic (red highlight) conducts retrograde via the slow pathway resulting in an inverted P wave (purple arrow). This now conducts to the ventricle (yellow highlight) with a prolonged PR interval, because the AV pathways are partially refractory.
Echo beats can set up a re-entry circuit, resulting in AVNRT.
AVNRT can be divided into typical (slow-fast) oratypical (fast-slow) as well as a number of rarer forms related to more than one slow or fast pathway with similar electrophysiological properties. On the ECG, they can be identified and differentiated by the positioning of the P wave in relation to the QRS complex, which in turn is related to the direction of the re-entrant AV nodal circuit. However, in about 60% of cases, the P wave is buried in the QRS/T and cannot be identified on the ECG.
Typical AVNRTis by far the most common of the junctional tachyarrhythmias(>80%) and most frequently occurs in young, otherwise healthy females. It starts abruptly, often provoked by dehydration, exertion, caffeine or alcohol. The tachycardia is frequently initiated by a premature atrial ectopic which finds the fast pathway refractory and conducts anterograde via the slow pathway. With an echo beat, a re-entry circuit may be created. The term slow-fast describes its movement in the AV node. As we have seen in our presented ECG, the ventricular rate of these tachycardias is dependent on the electrical properties of these pathways and is usually in the range of 140 to 260 bpm.
On the ECG, the conduction of the inverted P wave to the ventricle is via the fast pathway and hence the R-P timing is short. Consequently, the P wave may be embedded within or just beyond the QRS, creating a “pseudo” wave.
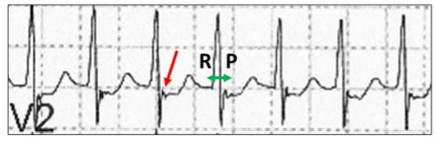
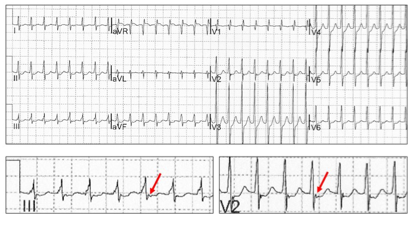
pseudo r’ wave best seen in V1 or V2 (red arrow). The R-P timing is short.
Pseudo-S wave in leads II, III, and AVF (red arrow).
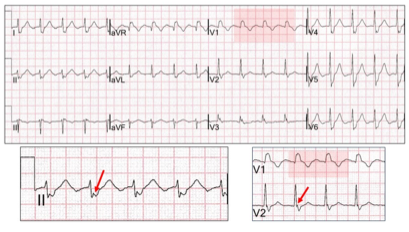
AVNRT in the young with short R-P interval and visible P waves (red arrows).
Because of the ventricular rate, aberrant ventricular conduction can occur or there may be an underlying bundle branch block. The widened QRS would be more likely to conceal the retrograde P wave but depending on the R-P timing, it may be possible to identify the P wave in leads where the QRS is not as broad (red arrows).
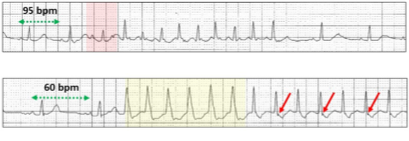
Aberrant ventricular conduction is dependent on the cycle length of the AVNRT as well as the long cycle and short cycle.
Above: Sinus rate 96 bpm, an atrial ectopic (red highlight) initiates a short run of AVNRT with narrow QRS.
Below: In the same patient, slow sinus rhythm (long cycle) and the atrial ectopic (short cycle) starts the AVNRT with aberrant ventricular conduction (yellow highlight). As the rate slows, the QRS complexes narrow, and a P wave is seen (red arrows).
Atypical AVNRT(10-16%)is usually initiated by a premature ventricular ectopic which finds the slow pathway refractory and conducts retrograde to the atria via the fast pathway and anterograde to the ventricles via the slow pathway, thereby creating a re-entry circuit. On the ECG, the conduction of the inverted P wave to the ventricle is along the slow pathway and hence and the R-P timing is very long and the P-R timing very short.
ECG, of a tachyarrhythmia which fulfills the criteria for an atypical AVNRT; long R-P and short PR intervals (green stippled arrows) but also could be interpreted as a junctional tachycardia.
No tricks. Just a selection of tracings from a Holter study.Look at each one carefully, use calipers, arrows and highlight and write down your conclusions.