To receive a free PDF copy of The Fundamentals of Electrocardiograph Interpretation by Harry Mond, subscribe to his email blog by entering your email address below.
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.
Purchase the textbook
Purchase a hard cover or paperback copy of The Fundamentals of Electrocardiograph Interpretation by Harry Mond on Amazon.
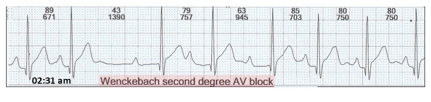
I came across this rhythm strip whilst reporting Holter monitor recordings.
What do you think?
There is:
Change in the PR interval
Pause
Is this enough to call the rhythm Wenckebach second degree AV block?
As the physiologist suggests Wenckebach AV block, let us start by revisiting the footprints.
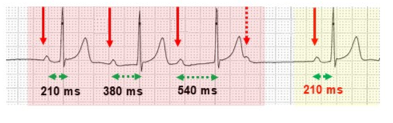
The typical features of Wenckebach AV block usually occur in sequences (red highlight).
Sinus rhythm (red arrows) with no alteration in sinus cycle.
Progressive increase in PR interval (green stippled arrows) called AV node fatigue.
Failure of AV conduction (red stippled arrow).
The AV node rests, and the next sequence (yellow highlight) commences after a pause.
The PR interval is shortest with the first beat of a sequence (210 ms).
When analysing and reporting Holter monitor tracings, Wenckebach AV block is very common. However, the typical findings occur <10% of the time. Rather the appearances are atypical and may be difficult to recognise. A means of instant recognition of Wenckebach AV sequences is to identify three absolute defining footprints.
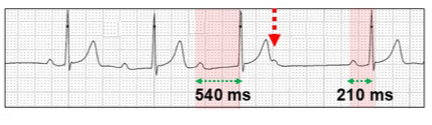
To summarize:
PR interval longest before the dropped beat (wide red highlight, 540 ms).
Non-conducted P wave (red stippled arrow).
PR interval shortest after the dropped beat (narrow red highlight, 210 ms).
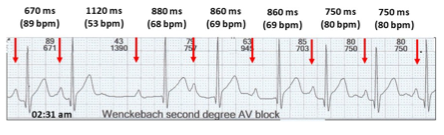
Now let us now review the tracing.
Sinus rhythm.
All P waves are conducted to the ventricle (no dropped beats).
Abrupt sinus slowing.
There are no absolute features of Wenckebach AV block.
Why sinus slowing?
Nocturnal heightened vagal tone.
Particularly in the young or athlete, heightened nocturnal vagal tone is parasympathetic cardiac stimulation and peripheral vasodilation. On the ECG, heightened vagal tone is seen as:
Sinus node - right vagal stimulation - abrupt sinus slowing, sinus pauses and atrial and ventricular escape rhythms as well as combinations of these.
AV node - left vagal stimulation - Wenckebach AV block.
Sinus and AV node features may occur separately or in combination creating bizarre, often difficult to recognise ECG rhythms. The features may not fulfill the absolute criteria of Wenckebach AV block.
Let us review some examples.
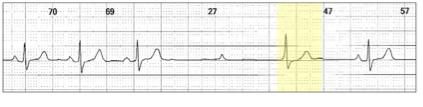
Abrupt sinus slowing (red arrows) with no PR lengthening (red highlight).
Abrupt sinus slowing (red arrows) with no PR lengthening. A junctional escape beat (yellow highlight) obscures the absolute Wenckebach AV block features.
The abrupt heightened vagal tone results in sinus slowing and an aborted Wenckebach AV sequence.
There is an attempted Wenckebach AV block sequence, but AV conduction continues albeit with a prolonged AV delay. As the heightened vagal tone subsides, the PR intervals shorten. This is called pseudo-reversed Wenckebach AV block.
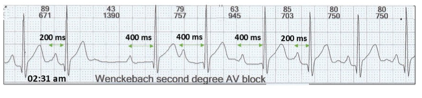
Now let us review the PR intervals.
There is a dramatic nocturnal change in the PR interval from 200 ms to 400 ms for three complexes and then reverts to 200 ms.
This is dual AV node pathways physiology with slow pathway onset.
Slow pathway conduction onset.
The transition from fast pathway to slow pathway assumes fatigue in the fast pathway usually due to increase in the heart rate, shortening of the P-P interval or the fast pathway is refractory.
Atrial ectopic.
Left: Atrial ectopic (red highlight, blue arrow) with short PR interval and atrial coupling interval of 800 ms.
Right: With shortening of the atrial coupling period to 700 ms, the atrial ectopic red highlight, blue arrow) would normally be non-conducted due to a refractory fast pathway. However, the ectopic now conducts through the slow pathway. Also consider concealed retrograde penetration of the proximal conducting system.
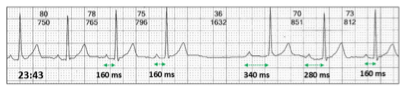
Wenckebach AV block pause.
Wenckebach AV block sequence (red highlight) with dropped P wave (red stippled arrow). The next dropped beat or block in the fast pathway (purple stippled arrow) allows slow pathway conduction (yellow highlight, 540 ms). Following the next non-conducted sinus P wave (red stippled arrow), there is a pause and fast pathway conduction is restored (blue highlight).
Understanding heightened vagal tone, abrupt attempted Wenckebach AV block, and dual AV nodal pathway physiology, what does our ECG show?
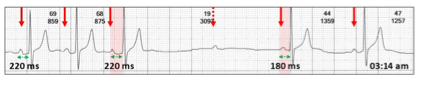
Sinus rhythm (red arrows).
Nocturnal heightened vagal tone with:
Abrupt sinus slowing (red highlight).
Unsuccessful abrupt Wenckebach AV block without previous PR prolongation.
There is an attempted dropped P wave (red stippled arrow) due to a refractory fast pathway and hence
Slow pathway conduction for three beats.
Vagal tone diminishes and fast pathway conduction recommences.
So the label of Wenckebach second degree AV block is at least partially correct.
It has been suggested that the pause may be due to a concealed non-conducted atrial ectopic. However, this is unlikely as the compensatory pause would not allow the fast pathway to block and thus allow slow pathway conduction.
No tricks. Just a selection of tracings from a Holter study.Look at each one carefully, use calipers, arrows and highlight and write down your conclusions.