To receive a free PDF copy of The Fundamentals of Electrocardiograph Interpretation by Harry Mond, subscribe to his email blog by entering your email address below.
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.
Purchase the textbook
Purchase a hard cover or paperback copy of The Fundamentals of Electrocardiograph Interpretation by Harry Mond on Amazon.
We now know that in some pacemaker recipients, pacing from the apex of the right ventricle may result in left ventricular dysfunction. In order to encourage normal atrio-ventricular conduction in pacemaker patients who do not require ventricular pacing such as the sick sinus syndrome, all pacemaker manufacturers now have programmable ventricular pacing minimization algorithms that effectively pace only in the atrium (AAI)but will automatically revert to dual chamber pacing (DDD) in the presence of failed AV conduction. Some of these algorithms are complex and all may result in bewildering ECGs, which may be incorrectly interpreted as pacemaker malfunction. The reason we suspect pacemaker malfunction with these algorithms is that the AV delays appear to violate what I call the “law of AV conduction”as it applies to dual chamber pacing.
The programmed paced AV delay(Ap Vp) is always longer than the sensed AV delay (Ap Vs). If AV conduction results in ventricular sensing, it is intuitive that it will occur before completion of the AV delay, unless it is a fusion beat.
Ventricular pacing minimization algorithms intentionally violate the law of AV conduction in order to promote ventricular sensing and they can be recognised on the ECG by the ventricular sensed AV delay being longer than with ventricular pacing. There are currently seven unique algorithms from 5 manufacturers, and most can be recognised on the ECG. These programmable algorithms can be divided into two broad groups, four convert from atrial to dual chamber pacing and three use AV hysteresis in the DDD(R) mode.As the name implies, AV hysteresis allows the AV delay to be extended beyond the programmed value in order to encourage ventricular sensing. The algorithm scan be very complex and there are frequent manufacturer software iterations. On the ECG, there is AAI(R) pacing in patients with intact AV conduction. AV conduction is continually being monitored and the presence of ventricular pacing indicates a change in pacing from AAI(R) to DDD(R) and is referred to as“mode conversion”.
Our ECG example is the most commonly recognised algorithm, the Medtronic managed ventricular pacing (MVPTM).In order to explain the ECG, let us review the Medtronic algorithm which is based on atrial paced timing.
Three lead Holter monitor recording. Atrial pacing (Ap) and ventricular sensing (Vs) with an AV delay of 300ms. Failure of AV conduction (red arrow) results in a ventricular pause of 1.6seconds. With the next Ap, rescue ventricular pacing (Vp) will occur after anAV delay of 80 ms (red highlight). The next Ap again allows for AV conduction and this time it is shortened to 260 ms, suggesting that the droppedAp was the result of Wenckebach AV block.
Similar ECG appearances occur with non-conducted atrial ectopics.
Ap Vs with an AV delay of 280ms. A non-conducted atrial ectopic results in a rescue ventricular paced beat with an AV delay of 80 ms (red highlight). Ap Vs then continues at 280 ms.
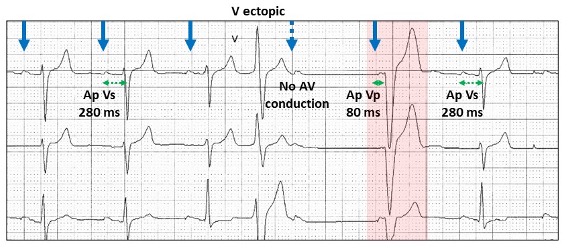
With a ventricular ectopic, atrial pacing depolarizes the atrium, but AV conduction may still be refractory, thus activating the algorithm.
Ap Vs with a conducted AV delay of 280 ms. A ventricular ectopic (V ectopic) is not sensed in the atrium and thus the next Ap will occur during the refractory period of the conducting system (blue stippled arrow). This is recognised as a dropped beat and thus the next Ap is followed by ventricular pacing (Vp) with an 80 ms AV delay. Ap Vs then continues with a 280 ms AV delay.
Let us apply the algorithm to our case.
AP Vs with a very long“non-physiologic” AV delay of 460 ms. With failed AV conduction, the next AV delay is not 80 ms (red highlight). This is because the next P wave is atrial sensed (As) and hence earlier in timing to Ap. Because the algorithm is atrial paced timing, the AV delay is extended. The stippled blue line indicates Ap timing with Vp 80 ms later. Because these patients have sick sinus syndrome almost always the timing is extended to Ap. This ECG appearance is rare and although I have seen the algorithm working about 50 times with Ap, this is the first time I have seen this with As.
We need to be able revert to DDD pacing to prevent frequent pauses. This will occur if two beats fail to conduct during a sequence of 4 atrial paced beats.
AAI (Ap Vs) with an AV delay of 400 ms. Two Ap fail to conduct (red 1 and 4). Following are two rescue Vp with an AV delay of 80 ms. The next Ap Vp has the DDD programmed AV delay of 200 ms. This will continue until there is a programmed conduction test to test the integrity of AV conduction. If AV conduction is intact, AAI pacing is re-established.
Unless you understand these algorithms, the ECG appearances suggest “serious” pacemaker malfunction.
No tricks. Just a selection of tracings from a Holter study.Look at each one carefully, use calipers, arrows and highlight and write down your conclusions.
I was asked to review this Holter monitor, the report of which stated: “Sinus rhythm, ventricular rate ~ 90 bpm, Wenckebach AV block”. What do you think?